


Recently the efficacy and safety of electroconvulsive therapy (ECT) in depressive disorders has been reviewed, and ECT was found to be effective in the short-term treatment of depression, ‘probably more effective than drug therapy’ (UK ECT Review Group, 2003). Patients’ perspectives on ECT have also been reviewed (Reference Rose, Fleischmann and WykesRose et al, 2003), and memory loss was highlighted as a particular concern. The American Psychiatric Association Task Force Report (2001) recommended that efforts should be made to minimise adverse effects during treatment. The National Institute for Clinical Excellence (NICE) published guidance on the use of ECT in April 2003 (National Institute for Clinical Excellence, 2003). It recommended that ECT is used only to achieve ‘rapid and short-term improvement of severe symptoms after an adequate trial of other treatment(s)… and/or when the condition is considered to be potentially life-threatening, in… severe depressive illness, catatonia and a prolonged or severe manic episode’. This recommendation is regarded as controversial and at odds with modern ECT practice by many psychiatrists. The NICE document states that the Committee took ‘special note’ of the evidence given by users relating to adverse effects and further notes that outcome measures should include user perspectives of treatment with ECT. We present here the results of users’ routine ratings of side-effects experienced during a course of ECT in one treatment clinic, and their ratings, after the course was completed, of aspects of the treatment procedure.
Methods
People who were receiving ECT were asked routinely by nursing staff to complete a side-effects form (ECT questionnaire 1) weekly during their course of treatment. The form listed five possible specified side-effects (memory difficulty, headache, confusion, dizziness and vomiting) and also a sixth category of ‘another side-effect which was…’. This list of side-effects was used in a previous study (Reference BenbowBenbow, 1988). For each possible side-effect, they were asked to circle one of four options: severe, moderate, mild and none. They were also asked ‘how much do you think ECT is helping you so far’, with a choice of four options: not at all, a little, moderately and a lot. Forms were returned to the ECT clinic in order that any side-effects could be taken into account during treatment.
At the end of their ECT course, a further questionnaire (ECT questionnaire 2) was sent to patients, either on the ward prior to discharge or by post following their discharge. This questionnaire consisted of two parts: part 1 asked patients to rate various aspects of treatment on one of five options: very unpleasant, slightly unpleasant, neutral, slightly pleasant or very pleasant. Part 2 asked three further questions: how much did the treatment help you (options: much worse, slightly worse, no different, a little better, a lot better), how was the treatment explained to you beforehand (options: not at all, very badly, rather poorly, fairly well, very well), and how did ECT compare with going to the dentist (options: much worse, slightly worse, no different, a little better, a lot better).
Results
Four hundred and thirty-four side-effects forms were collected (a mean of almost five forms per course), giving information on 90 courses of ECT given to 70 individuals (one person received six courses, three received three courses and nine received two). Over 95% of people were receiving ECT for a depressive disorder: their ages ranged from 16 to 91, with a mean of 64 years. For 12 courses of ECT (13%), the patient did not report any side-effects at all. Fifty-four copies of ECT questionnaire 2 were received.
For each of the six side-effects, a mean score was calculated for the whole course by adding the scores on all forms returned for that course and then dividing the sum by the number of forms returned. For reported memory problems, 29% of respondents had a mean score of 0 across the course as a whole, indicating that they did not report memory difficulties on any of the returned side-effects forms for that course. Fifty-two per cent of respondents had a mean score for memory problems between 0.1 and 1.0. This could be achieved by reporting mild memory problems (scoring 1) on each form or by scoring more severe memory problems (moderate or severe) on some of the forms returned. Nineteen per cent of respondents scored above 1 and below 2 on memory problems, and no one scored more than 2. Figure 1 compares the scores for all six side-effects. In contrast with Figure 1, which illustrates side-effects across the course as a whole and their severity, Table 1 sets out the percentage of people who reported a side-effect as severe or mild/moderate at any stage of their treatment.
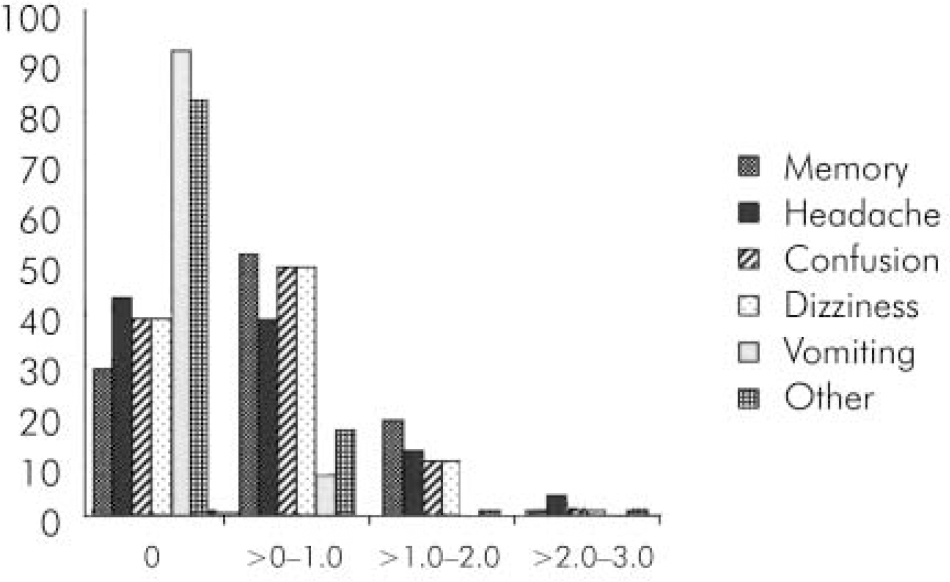
Fig. 1. Average rating score for six listed side-effects over a course of ECT.
Options were scored as follows: severe 3, moderate 2, mild 1, none 0. For each individual an average score was calculated by adding the score for each side-effect across the course, and dividing it by the number of forms returned. This gave an average rating score for each side-effect for each person treated. Shows percentages of patients whose average side-effects rating falls into each of scoring bands: 0 side effect not reported, >0-1.0 mild, >1.0-2.0 moderate, >2.0-3.0 severe.
Table 1. Percentage of people treated with electroconvulsive therapy (ECT) who reported a severe or mild/moderate side-effect on any side-effects form related to each of 90 courses of ECT*
| Side-effect | Severe (%) | Mild/moderate (%) |
|---|---|---|
| Memory problem | 10 | 62 |
| Headache | 11 | 44 |
| Dizziness | 10 | 52 |
| Confusion | 3 | 41 |
| Vomiting | 0 | 9 |
| Other** | 7 | 11 |
The ECT staff and ‘falling asleep’ (Table 2) were aspects of the treatment procedure that were given a positive rating by most respondents. ‘ Waking up’ was the only treatment aspect rated negatively by 50% or more of the respondents, although few people rated the waiting period, the anaesthetic injection and the recovery period positively.
Table 2. Patients’ ratings of different aspects of electroconvulsive therapy (ECT) at the end of their treatment course (n=54)
| Very unpleasant (%) | Slightly unpleasant (%) | Neutral (%) | Slightly pleasant (%) | Very pleasant (%) | |
|---|---|---|---|---|---|
| Waiting | 11 | 35 | 44 | 6 | 2 |
| ECT staff | 2 | 2 | 4 | 9 | 83 |
| Anaesthetic injection | 13 | 35 | 39 | 9 | 4 |
| Falling asleep | 0 | 9 | 39 | 13 | 39 |
| Waking up | 6 | 44 | 30 | 11 | 7 |
| Recovery period | 2 | 37 | 39 | 11 | 11 |
| Much worse (%) | Slightly worse (%) | No different (%) | A little better (%) | A lot better (%) | |
|---|---|---|---|---|---|
| It made me | 0 | 2 | 9 | 37 | 48 |
| Compared with the dentist | 6 | 11 | 44 | 20 | 7 |
| Not at all (%) | Very badly (%) | Rather poorly (%) | Fairly well (%) | Very well (%) | |
|---|---|---|---|---|---|
| How was the treatment explained? | 2 | 6 | 6 | 52 | 26 |
Most people (85%) rated themselves as a little or a lot better at the end of the course of treatment. It was more common for people to find ECT a little or a lot better than going to the dentist (27%), than to find it much or slightly worse (20%). Most people (78%) thought that the treatment had been fairly or well explained.
Discussion
This was initially designed as an audit. However, in view of the NICE recommendations, its findings are important and merit dissemination. The side-effects forms were returned to the ECT clinic staff in order that action could be taken to alleviate side-effects where possible, and were not returned anonymously. Actions taken depended on discussion between patient, ECT clinic staff and ward staff. If a person reported headaches, they would be offered treatment for this after subsequent treatments. If confusion or memory problems were reported, the ward doctor was asked to review concurrent medication as a first step. However, if the problem persisted, a change from bilateral to unilateral treatment or an increased inter-treatment interval might be recommended. Returns of questionnaire 2 (relating to 60% of treatment courses) were lower than questionnaire 1, but people were often discharged soon after completing a course of treatment, and therefore had less of a chance to complete the questionnaire.
One criticism of our method of monitoring side-effects is that it may have increased people's reluctance to report side-effects, since they were reporting them to the staff responsible for their treatment. Patients were actively encouraged to report any problems in order that action could be taken to alleviate side-effects, and in an endeavour to avoid under-reporting. However, Rose et al (Reference Rose, Fleischmann and Wykes2003) reported that satisfaction tends to be higher when clinic staff members, rather than a fellow service user or neutral person, administer questionnaires. This might have led to under-reporting of side-effects and poor outcomes. A further possible factor, which may have led to over-reporting of side-effects, is that people rated as side-effects symptoms that their treatment teams regarded as being no different from those experienced prior to treatment. These are considered to be depressive symptoms or side-effects of concurrent medication. This was taken into account in deciding what action to take in response to side-effects ratings, but is not reflected in the raw results. Although side-effects were commonly reported, they were predominantly rated as mild. Only a small proportion of people reported any moderate or severe side-effects. Our findings provide potentially useful information regarding patients’ experiences during treatment, which can inform the discussions with people who are considering having ECT and their families.
In future, people who are about to start a course of ECT will be asked to rate the symptoms, which were listed as possible side-effects of treatment, prior to receiving ECT. This is because some individuals were recorded in their case notes as complaining of a symptom before receiving treatment, and it was regarded by their ward team as being a symptom of depressive illness (e.g. headaches) rather than a side-effect of ECT. It is more difficult to tease out the effect of ECT on an established symptom during a course of treatment. It would also be useful to record how often treatment is changed as a result of side-effects monitoring. Feedback on wider aspects of the treatment from people who have received ECT could usefully be incorporated into planning policies and procedures in the clinic, in order to minimise waiting times, and to make the recovery period as comfortable as possible, for example.
We recommend that people who are receiving ECT should be encouraged to feed back to staff their subjective experiences of treatment, and to rate the occurrence and severity of side-effects. This does not remove the need for staff to monitor side-effects objectively (e.g. by standardised memory tests), but provides a fuller picture and allows changes to be made to treatment techniques and procedures where appropriate. Furthermore, we recommend that consideration should be given to patient follow-up after completion of treatment, with a questionnaire designed to assess longer-term side-effects and outcome.




 Open access
Open access
eLetters
No eLetters have been published for this article.